




Did The FDA Mess Up With Aduhelm?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Today I have a new post and discussion question.
To reiterate the rules:
I’ll pose a question and give my thoughts if I have any. In a future newsletter I’ll include ~3 of my favorite answers people reply with. I’ll possibly even make a meme related to your answer.
Good answers are ones with a novel viewpoint, data to back up their claim, personal stories, and avoid clearly shilling something.
Please reply to this email with your thoughts on the question and let me know if you want to have your name or be anonymous. You have to actually be on the newsletter to submit a reply to it obviously.
Try to keep answers to 2 paragraphs or less please. This obviously doesn’t apply to me because it’s my newsletter and these are house rules.
What are your thoughts on the FDA’s recent approval of Biogen’s drug Adulhem?
Recently, the FDA approved a new drug from Biogen for Alzheimer’s disease called aducanumab (marketed as Aduhelm). This is basically the only new therapy that’s been approved for Alzheimer’s in nearly two decades.

Background
Aduhelm is one of 20+ drugs in development that is based on the amyloid cascade hypothesis, all of which have names that sound like a jazz musician scat singing (bapineuzumab, solanezumab, etc.). The hypothesis suggests that a buildup of beta-amyloid plaques in the brain is the cause of Alzheimer’s. Aduhelm targets and clears out those plaques, but is the only drug so far to make it to the FDA after almost every other drug failed or stopped development.
A few key things about the drug and the trial:
The sponsor ran two identical phase III trials with the drug. Both trials were looking to improve something called the Clinical Dementia Rating Scale - Sum of Box Scores (a way you measure the progression of some neurodegenerative disorders and cognition) in patients with mild Alzheimer’s. One of the trials didn’t detect any improvement in patients compared to the placebo arm, and both trials were stopped in the middle. However, Biogen went back through the data and found that the other trial did show some improvement once the remaining patients finished the trial. Both trials did show a decrease in amyloid plaques based on brain scans.

The drug wasn’t without side effects. Safety data from the two trials showed that more than a third of patients on the drug experienced amyloid-related imaging abnormalities (ARIA). Many of the patients had no symptoms of mild systems, but 6.2% of participants receiving the high dose ended up stopping the drug, some got brain bleeds, and one died.
The FDA brings in an advisory committee to look through the data on drugs that are difficult to come to a judgment about. The advisory committee for this drug nearly unanimously agreed it should not be passed (one person said “idk”, but more formally). In general, the FDA disagrees with the advisory committee about ~22% of the time and most of the time it disagrees in order to be more restrictive than the committee suggests.
The FDA gave the drug an Accelerated Approval. This type of approval aims to bring therapies to market more quickly when there aren’t many options for a given disease. It does this by looking at how well a drug affects “surrogate endpoints”, things that are measurable that can be reasonably connected to an improved clinical outcome later. For example, tumor size would be considered a surrogate endpoint since shrinkage of the tumor likely means that a person’s health is going to improve. Or brain wrinkles might be considered a surrogate for getting off Twitter. In this case, the surrogate endpoint would be “reduction of the amyloid plaques'' which the agency/Biogen believes is a predictor of improved cognitive or functional outcomes for Alzheimer’s patients.

Biogen is running a confirmatory trial within the next 9 years to prove it reduces the amyloid plaques over a long period of time and slows cognitive decline. The company can continue to sell the drug during this time, and it seems like the FDA is pushing the company to finish the confirmatory trial sooner than later. We don’t have a great record of getting companies to submit this confirmatory data on time, but with so many eyes on this drug it’ll be hard to slip under the radar.
It’s worth noting that the Accelerated Approval of the drug is for any severity of Alzheimer’s though the drug was only evaluated in mild-moderate patients during the trial.
Biogen is setting a list price of the drug at $56K per year, not including the additional imaging + visits that are required. It is an infusion drug that would be covered by Medicare Part B, which covers drugs that need to be administered in a physician setting (generally ones you can’t give yourself).
To understand how large the delta in pricing expectations is, ICER (a well-respected non-profit that evaluates drug cost-effectiveness) believes the price should be between $2500-$8300/year. The report is worth a read, even if you disagree with the pricing methodology (which many folks do).
---
{{interlude 4}}
My thoughts
So that’s enough background. Let me start by saying I am not a scientist, and so I can’t really evaluate much about how the drug works (aka. the mechanism of action) or the amyloid hypothesis generally.
But I think it’s actually good that this Biogen fiasco has happened because it exposes the disconnect between drug approvals, coverage, and reimbursement by providing the most extreme example possible. We seem to be approving drugs with questionable efficacy with slightly higher price tags and not a lot has been done to address it. But now we have such a whammy that it’s impossible not to address it.
Here’s the issue: an FDA approval today is divorced from comparing whether a drug is cost effective or not. The role of the FDA is to determine the safety and efficacy (aka. “does it actually work?”) of a drug. If the data shows that, the FDA’s job is to give a greenlight, and then the pricing is someone else’s problem.
By itself this isn’t an issue - the FDA focuses on whether the drug works/is safe and then the insurance market decides if it’s worth covering and how much to reimburse. However the reality is that FDA approvals now live on a spectrum of “definitely works well” to “seems to potentially work, we’ll approve and see what happens”. Yet reimbursement of these drugs does not seem to have a sliding scale to account for this spectrum. The usual course of action is to set up obstacles and hoops to jump through before patients can access the drug.
This is most apparent in Medicare, which is where most of Aduhelm’s target patients are covered. Medicare has no ability to negotiate down the price of the drug with manufacturers. Medicare Part B (which would cover Aduhelm) has to cover any drugs that are deemed “reasonable and necessary” according to a three prong evaluation:
- The drug has to be safe and effective
- The drug can’t be experimental or investigational
- The drug has to be appropriate for Medicare patients
Despite not being able to negotiate price, Medicare Part B does have some flexibility in deciding WHO gets covered. There’s a ton of nuance here about the difference between creating a federal standard for coverage vs. local determinations of coverage and if you care about the details I recommend reading this piece. But the general gist is that the determination is WHO should get the drug and not how much exactly the payment should be.
This is also complicated by another dynamic when it comes to Medicare Part B. Hospitals and doctors are actually incentivized to give this drug because most doctors are paid the drug’s Average Sale Price + 6%, so more expensive drugs are better for them (not even including the money they’ll get from more imaging).
In summary, everyone does well here but Medicare and as a proxy the taxpayer. The predominant tool against this is setting up coverage restrictions, which will understandably make a lot of people affected by Alzheimer’s extremely upset. During a time where Medicare is scheduled to go bankrupt within the next few years, we’re approving a drug that is potentially going to cost more than Medicare pays for every other drug combined in the part D program and blows the highest spending Part B drugs out of the water.

This doesn’t even get into the other issues of this approval:
- It was approved for any severity of Alzheimer’s, which is beyond the patient population studied in the trials
- Being the only Alzheimer’s drug that’s been approved recently, patients are stopping enrollment in other trials for potentially better drugs and flocking to this one
- Other drugs that have failed are looking at this approval and saying “hold up, even our data was better than this” and now trying for their own approvals
- No one is sure how long to put patients on this drug since the phase III trial was never finished
- The drug is so expensive that patients will probably hit their out-of-pocket maximum for drugs or need supplemental insurance to be able to pay for it (which will be tough for many lower income people)
- This is going to totally wreck Medicaid which will have to cover it for their 65+ year old members but can’t just print money to solve their problem
- At a time where people’s faith in clinical trials, authority figures, and the ability to evaluate treatments is shaky we’re introducing one of the most mixed message drugs into the market

So to me, the approval seems bad for all of the above reasons, but it can potentially be the final straw that pushes us to a new paradigm for how we think about drug approvals and drug pricing.
For one, maybe this is what finally pushes the public/politicians to allow Medicare to directly negotiate with drug manufacturers. This has pretty much bipartisan support. Sure there are probably tradeoffs to letting this happen, but I think on net we’d get more cost effective drugs.

Two, maybe this will allow us to push more meaningfully into value-based contracts with drug makers. This would be especially helpful for drugs with high price tags that relied on surrogate endpoints for approval but the final clinical benefit still needs to be evaluated. This idea has been pitched and almost never followed through, but with drug costs getting this egregious maybe it’s finally time.
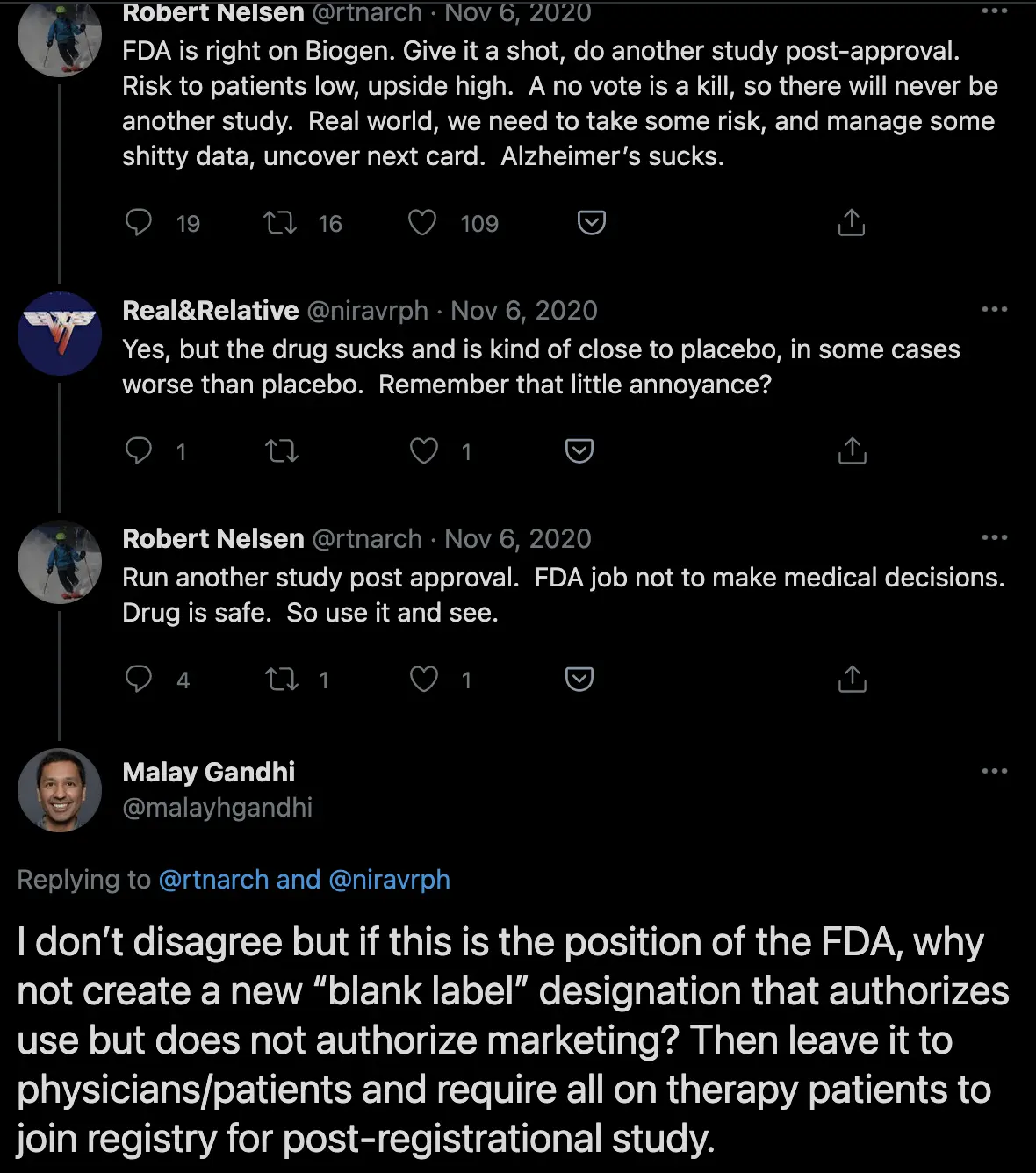
Finally, maybe we can rethink what should go into an FDA approval or what the concept of an FDA approval means. This idea was interesting where we introduce a new blank label designation instead of a binary “pass and allow total coverage and marketing vs. no pass and killed”. Maybe there’s a cap on the profit a company can make on a drug while it’s still in a real-world study. Smarter people than I have suggested using something called “coverage with evidence development”, a tool CMS can use to only cover patients that take part in a clinical trial to learn more about the drug while it assesses whether to give full coverage or not.
I’m not sure the right path, but with the ability to do meaningful real-world evidence studies we should get more exploratory with what a spectrum of approvals might look like instead of sticking to this very binary process for coverage. The number of therapies with extremely high price tags is only going to get higher, but we need a way to evaluate and pay for these drugs differently if they’re high priced miracle drugs (like one-shot hepatitis C cures) vs. high-priced drugs with questionable results (like Aduhelm).
Someone framed this to me as “what if we spent an extra $56K per Alzheimer’s patient on caregiving as the comparison instead” to see if that improves lifestyle/symptoms more. I’d be curious what that looked like too.
Anyway, most people seem to have this opinion so particularly interested in anyone that has a convincing case FOR the drug.
Thinkboi out,
Nikhil aka. "Accelerated Disapproval"
Twitter: @nikillinit
Thanks to Malay Gandhi for feedback on this post (twice)
---
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
But first…DATA CAMP APPLICATIONS CLOSE SOON
See All Courses →If you’re into healthcare data and want to be around other healthcare data nerds, you really should apply to Data Camp ASAP!! The people are saying nice things about it because we do a lot of really awesome workshops to make you better with healthcare data.
Applications are due 4/24, BUT YOU WILL FORGET SO DO IT NOW IT TAKES LIKE 5 MIN IF YOU’RE SMART.
And sponsors…we’re already talking to people and have a limited number of slots. Hit me up if you want to see the packet.

And if you’re REALLY a healthcare data nerd…you’ll want to come to our AI x Risk Adjustment FREEEEE course. You’ll learn at least a thing or two, and probably a lot more. Starts 4/22 (aka…right before data camp applications!)
Quick Interlude - Data Camp Applications Due Soon!!
See All Courses →Don’t forget…DATA CAMP IS COMING TO YOU THIS JUNE! Applications are due 4/24, but fill it out now before you forget.
More details on the site. It’s all breakouts, a small curated group, and focused on tactical things to bring to work on Monday.
We’re also taking our first sponsors now - so if you want to get in front of data engineers/healthcare data pros, let us know.

Quick Interlude - Data Camp Applications Due Soon!!
See All Courses →Don’t forget…DATA CAMP IS COMING TO YOU THIS JUNE! Applications are due 4/24, but fill it out now before you forget. More details on the site. It’s all breakouts, a small curated group, and focused on tactical things to bring to work on Monday.
We’re also taking our first sponsors now - so if you want to get in front of data engineers/healthcare data pros, let us know.

Get Out-Of-Pocket in your email


