




Yet Another Teladongo Take
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Let’s get past how funny the word “Teladongo” is, because that alone took me 5 days and honestly I still sort of chuckle at it.
There’s already been a lot of coverage of the Teladoc-Livongo merger, so I won’t rehash the basics. Teladoc provides on-demand video or phone call visits to patients that have primary/urgent care issues. Livongo is a diabetes management company that uses a glucometer, some alerts + nudges, and coaches to help patients manage their diabetes (and other chronic disease issues).
The gist of most takes around their merger is:
- It is shaking up the market (lol)
- The combined Teladongo can address acute, chronic, and specialty care issues. Teladoc customers can potentially act as top of funnel to Livongo’s chronic care programs, and then layer in the specialty care via Teladoc (via their acquisition of InTouch) as necessary.
- There’s only 25% customer overlap, so there’s a lot of cross-selling and upselling that’s likely going to happen. Teladoc has a presence around the world, which Livongo can potentially use to expand past the US
- The combined entity covers >70M lives in the US
- Both of these companies were valued stupid highly already so this is all funny money. Livongo probably sold cause they realized it would be an infinite amount of time before their business caught up to their valuation and someone was willing to pay for it now. Teladoc realized their stock was also super pricey and they could use that to buy their way into the chronic care side since their current business isn’t great (which I’ll talk about later).
- Both companies basically acquired their way into their empires, so this combined entity with very highly valued stock will likely continue their acquisition trend post-merger.
- Teladoc has acquired more than 10 companies, including InTouch to get into specialty care and several international providers to get into other countries (BestDoctors, Advance Medical, etc.)
- Livongo basically began as an acquisition of a glucometer, EosHealth. The company then acquired into mental health via MyStrength and I’m sure will want to do the same with other areas of high spend for self-insured employers (musculoskeletal disease, maternity, etc.)
- Optum is absolutely bugging right now, and I’m sure they’re making a market landscape of every chronic care management company and figuring out who they can buy. Expect them to acquire some companies in the next year.

Instead of focusing on this transaction specifically, I think this really signifies an end of an era. The era where we had standalone telemedicine companies and the value prop was getting a video call whenever you needed it.
Teladoc = near flawless execution
My core belief is telemedicine is a commodity. Anyone can spin up some webRTC app and build a telemedicine application.
When I was just starting out as a healthcare analyst one of my first reports was looking at telemedicine. Parts of the report are cringeworthy to read now, but I remember looking into Teladoc and thinking about how weird it was that their utilization was so low but they seemed to be doing relatively well.

I couldn’t understand why Teladoc was doing well, and honestly years later I still didn’t. There were like a million different telemedicine companies (MDLive, DrOnDemand, American Well, etc.)
So obviously I asked Twitter, and I got some good answers.
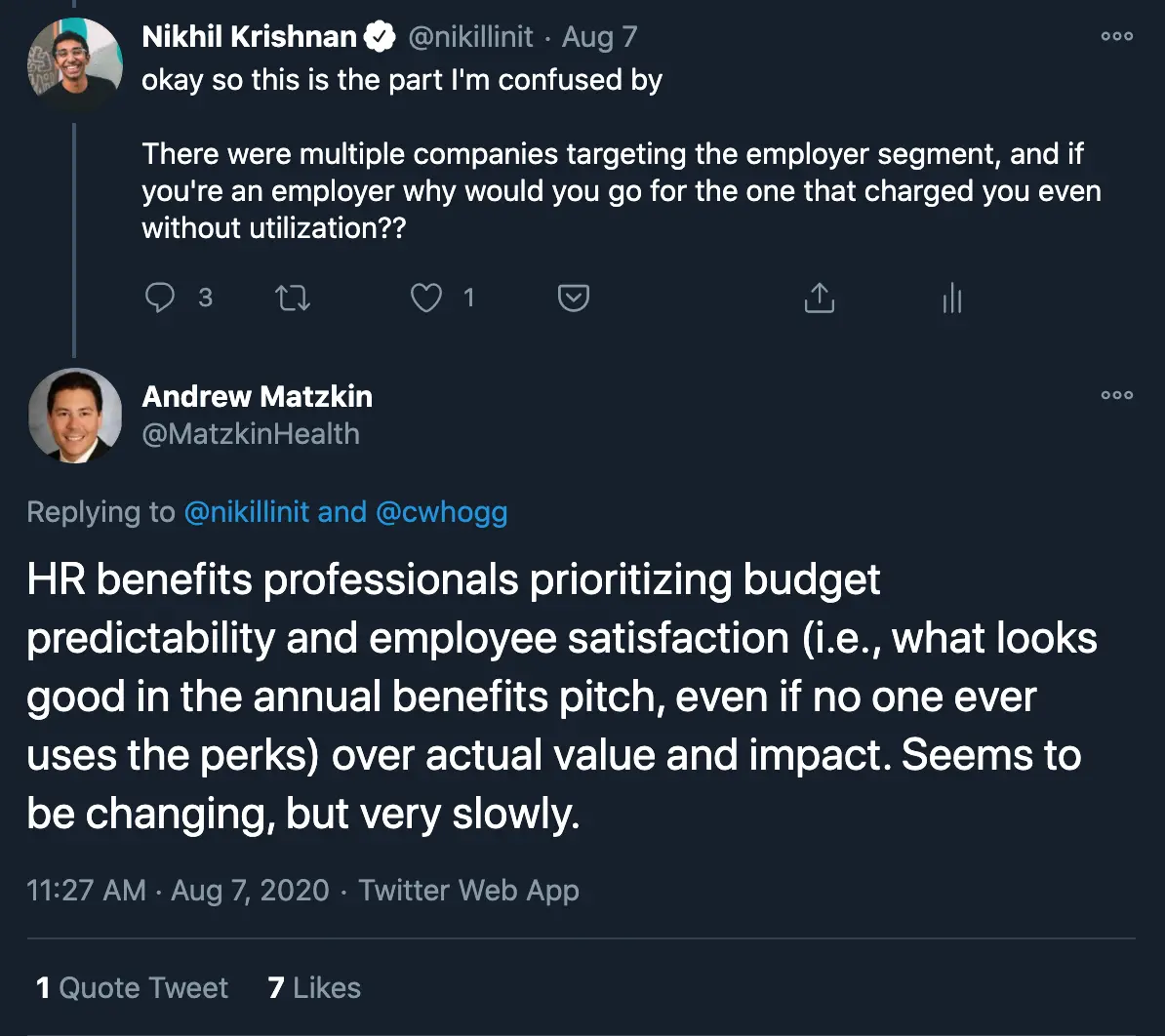
There are a few ways to differentiate yourself if your product is a commodity in a B2B sale:
- You hire sales people that have a deep rolodex and relationships. This is expensive but it works. Many of the success stories in v1 digital health companies have a founding team member as an ex-VP or above at [insert big name healthcare giant] which helps a lot.
- You make the deal terms themselves more attractive to the end buyer. Lower or more predictable pricing, different metrics you’ll charge for, etc.
- You strike some key distribution deal to become a preferred vendor of all the commodity services
- You build other things that you can bundle together with the commodity service that are not commodities
I forgot about my own lecture about selling in healthcare - the customer in most of these scenarios is risk-averse and cares more about predictability than effectiveness. Teladoc’s sale worked because even though most of the members signed up were not using the service, being charged per member per month meant you knew exactly how much you were going to be paying.

Plus, they struck key deals to become the preferred vendor for companies already selling to employers (Teladoc + Willis Towers Watson and Mercer on the benefits side, Teladoc + Aetna for their members and employer clients, etc.). From there, they went on an acquisition spree to grow their business. This was almost flawless execution so absolute respect to them.
However you can only be a commodity service for so long. At a certain point you have enough members that the line item is large enough that you start to wonder what you’re paying for, and only 5% of people using it doesn’t look great. That’s why Teladoc’s blend of new deals started seeing more and more focus on paying on “visit-fee only” aka pay-per-visit, instead of per-member-per-month even if no one uses it.

The other thing with commodities is that more people realize they can get in on the action pretty easily. Payers and providers are realizing that everything that happens AFTER the telemedicine visit (aka. where the patient gets in-person care next) is really important to them. So now payers and providers can offer their own white-labeled telemedicine solutions AND it comes with added benefits like $0 co-pays or transition to in-person care when necessary.
So…what do you do if you’re a commodity telemedicine services provider if you want to become more valuable? One way is expand geographically, which Teladoc did through many international acquisitions.
But domestically, turf seems to be heating up. Connecting a physician with a person over a video call doesn’t really seem to be a standalone business anymore.
From Telemedicine To Virtual Hospital
So if you’re Teladoc and you have these lucrative B2B contracts what do you do? Well you probably want to target the other high spend areas your customers have to deal with, namely chronic disease. Plus those patients have the nice added benefit of being much more engaged patients (Livongo had about ~35% eligible enrollment rate for potentially recruitable employees), which helps when you want to point to the fact that your solutions are actually being used.
So it’s not surprising that the disease areas highlighted are high spend categories where benefits brokers need to “check the box” that they have a solution for self-insured employers. From the merger presentation.

But more importantly, there’s now a virtual solution that’s a one-stop shop and already has aggregated the demand of >70M patients, which is more than any single company including UnitedHealth. Plus, it’s low friction and consumer-friendly. When you combine these together, Teladongo has some serious patient steerage capability.
However, moving into chronic care management is a very different beast than non-emergency acute issues. This raises two issues.
The first is that Teladongo is still missing the online-offline handoff, which completes the full loop of primary care and no telemedicine has really done that well. In chronic care this is really important because certain tests are difficult to do if you’re not in-person (e.g. checking for diabetes-related complications like diabetic retinopathy, certain tests that patients won’t be able to administer themselves, etc.).
That’s why I think a next step for the company will be routing patients to lower cost care settings when they need in-person care or ancillary services.
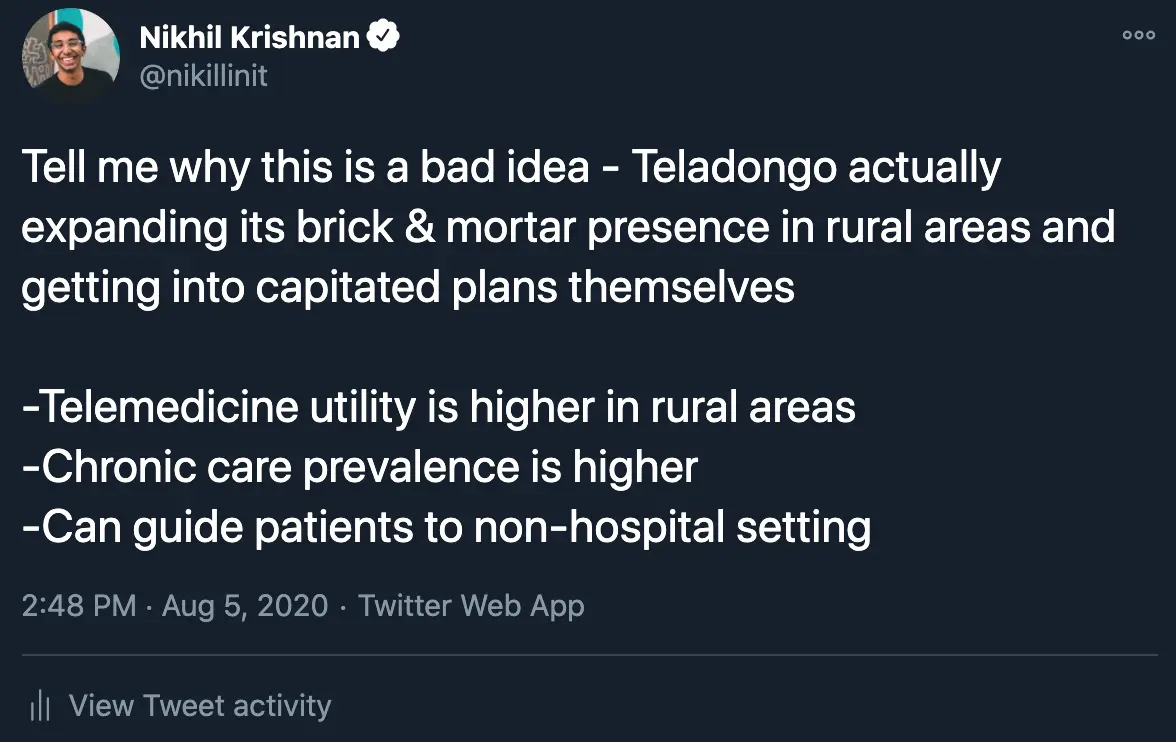
I’ve been convinced that this is a bad idea for them to build clinics themselves “beCaUsE oF tHE mARGiNs BrO” (which, as a side note, doesn’t seem to be an issue). But would it make sense for them to partner with someone like Walmart or other non-hospital settings through a partnership? I think so.
The second issue of building a chronic care company is that you can’t serve every master, aka. sell into every single type of healthcare company. Right now both Teladoc and Livongo are trying to sell into health systems, health insurance, employers, and patients.
Selling a white-label solution into a health system to enable their providers to use telemedicine is a completely different business than providing ongoing care to the employees of a company. Selling a white-label solution is about figuring out what the custom solution should look like for that health system, assessing the implementation steps, integrating third party data feeds, training staff, running system tests regularly, communicating internally/externally on how the system works, setting up regular reports and surveys of usage after rollout, etc. This is where American Well positions themselves, which you can see in their case studies and implementation checklists.
Chronic care management is more about figuring out how to get patients to use your product, getting supplies to patients and refilling those supplies in a timely fashion, monitoring patients and interpreting incoming data properly, assessing patient’s risk and escalating appropriately, training coaches and creating tooling for them, etc. Extremely different operationally + metrics of determining success.
But aside from the fact that these are two very different businesses, every single company in healthcare wants to own the “front door” of healthcare and be the point of contact for patients when they need anything. But they all want to be the point of contact so they can guide patients in a way that’s best for THEM, which is why you can’t sell that same solution to all of them.

I assume the combined entity is going to have some tension going forward selling into health systems and larger health insurers. Since employers don’t care about owning the “front door” themselves, this would likely be where they double down and expand.
But honestly that might be a good thing! One of the reasons it’s so hard to compete with hospitals is because they basically own all of the patient demand. Trying to get a patient to switch to your no name practice is tough. But now there’s a company that’s actually managed to pull off aggregating patient demand from the employer side - hopefully they actually use their positioning as leverage against hospitals and enable the longer tail of non-hospital settings by driving patients to them for in-person care.
{{interlude 3}}
Telemedicine Workflows and Parting Thoughts
Telemedicine 1.0 was about getting the face-to-face visit online and people focused on how it would make it more accessible for people that found it difficult to physically get to in-person care.
But the real promise of telemedicine is to create entirely new workflows, triage the kinds of labor used, and actually change the economics of visits.
Many companies use asynchronous telemedicine (texting, forms, etc.) to make it possible to scale the number of patients each coach/doctor sees and scale down the cost per visit.
Other companies use telemedicine to create proactive care workflows - reaching out to patients when something is wrong instead of waiting for a patient to reach out themselves. Watch detects atrial fibrillation? Cardiologist can check it remotely and ping you that there’s an issue before you feel anything yourself.
If we’re not changing the economics of a visit with telemedicine, we’re not actually figuring out ways to lower cost for the system we’re just making it easier for people to pay into it.
That’s also why I have very mixed feelings about the new telemedicine parity regulations where telemedicine visits are reimbursed the same as face-to-face visits. This removes the forcing function for the system to figure out how to reduce costs by making the economics of a visit work out with new telemedicine modalities. Now it’ll just be a bunch of people shifting the face-to-face visit to an online face-to-face visit.

Maybe getting all the providers and patients to even use telemedicine in the first place is the first step, so you reimburse them a lot first to even build out the telemedicine capabilities AND THEN you downgrade the payment once it’s a normalized behavior for patients. IDKKKKK.
Anyway this turned into a general rant about telemedicine. The rise of Teladoc is really a story about how to truly execute a sales & distribution strategy and make very smart acquisitions. Hopefully the story of Teladongo will be one of leveraging telemedicine to change the economics of primary care management for a broad swath of the population (hopefully beyond just employers).
And hopefully they for real go into the market as “Teladongo”.
Thinkboi out,
Nikhil
Twitter: @nikillinit
Thanks to Malay Gandhi for helping to push and shape my thinking in these areas
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


